![]()
![]()
![]()
![]()
![]()
![]()
![]()
![]()
REVESCO. Revista de Estudios Cooperativos. ARTÍCULOS
e-ISSN: 1985-8031
Pedro José Ponce Lozano
Universidad del País
Vasco UPV/EHU y ASISA (España) ![]()
![]()
Leire San José
Universidad del País
Vasco UPV/EHU (España)
![]()
![]()
José Luis Retolaza
Universidad de
Deusto (España)
![]()
![]()
https://dx.doi.org/10.5209/REVE.97314 Recibido: 07/06/2024 • Aceptado: 14/09/2024 • Publicado: 04/10/2024
ES Resumen. El sistema sanitario es considerado de primera necesidad. A pesar de contar con un sistema sanitario público, el sector privado lo complementa debido a las ineficiencias del sistema público. La contribución del sistema público se basa en el valor que genera para los stakeholders. La presencia de cooperativas en el sector sanitario es un tema poco investigado, pero de gran interés. En este estudio, se examina un caso de cooperativa de salud para identificar a los stakeholders beneficiados, el tipo de contribución realizada y cómo se apoya a la sostenibilidad y al Sistema Nacional de Salud. A través del análisis de este caso, se concluye que múltiples stakeholders están implicados, incluyendo empleados, proveedores, medios de comunicación, el grupo cooperativista, pacientes, administraciones públicas, instituciones profesionales y medios de transporte. Se resalta que el grupo cooperativista, inexistente en hospitales públicos, implica que los propietarios son stakeholders activos, situando al hospital en un punto intermedio entre lo público y lo privado, donde el lucro no es el objetivo principal.
Palabras clave. Valor social, stakeholders, generación de valor, mapa de stakeholders, valores cooperativos, no lucrativos.
Claves Econlit. I10, L30.
ENG Moncloa University HLA Hospital: the health cooperative contributing to generating value for stakeholders
ENG Abstract. The healthcare system is considered to be essential. Despite there being a public healthcare system, the private sector complements it due to inefficiencies in the public system. The contribution of the public system is based on the value it generates for stakeholders. The presence of cooperatives in the healthcare sector is a little-researched but highly interesting topic. This study examines a case of a health cooperative to identify the stakeholders who benefit, the type of contribution made, and how it supports sustainability and the Spanish National Health System. An analysis of this case concludes that multiple stakeholders are involved, including employees, suppliers, media, the cooperative group, patients, public administrations, professional institutions, and transportation services. Particularly noteworthy is that the cooperative group - which does not exist in public hospitals - means that the owners are active stakeholders, positioning the hospital between public and private sectors, where profit is not the primary goal.
Keywords. Social value, stakeholders, value generation, stakeholder map, cooperative values, non-lucrative.
Summary. 1. Introduction. 2. Theoretical framework: stakeholder perspective and social economy in hospital settings. 3. Methodology. 4. Results. 5. Conclusions, limitations and future lines of research. 6. References.
How to cite: Ponce Lozano, P.J.; San José, L. & Retolaza, J.L. (2024). Moncloa University HLA Hospital: the Health Cooperative Contributing to Generating Value for Stakeholders. REVESCO. Revista de Estudios Cooperativos, 148(1), 1-15, e97314. https://dx.doi.org/10.5209/REVE.97314.
The healthcare system is universally acknowledged to be a fundamental necessity, underpinning the well-being and health of populations worldwide. While public healthcare systems are prevalent, their inherent inefficiencies often require the support of the private sector to meet the comprehensive needs of society. This synergy underscores the critical role of healthcare systems generating value for stakeholders, extending beyond mere service provision to include community benefits and broader social value.
Healthcare cooperatives present a unique model, blending public service ethos with private sector efficiencies, aimed at addressing gaps in healthcare delivery. Despite the significant contributions of healthcare cooperatives, this area remains under-researched, particularly as regards their impact on stakeholders. These cooperatives not only provide essential medical services, but also foster a sense of ownership and responsibility among stakeholders, including employees, suppliers, patients, public administrations, and the wider community.
The primary research problem addressed in this study is to identify how healthcare cooperatives generate value for their stakeholders and contribute to the sustainability of the healthcare system, particularly the Spanish National Health System (SNHS). The literature on cooperatives in the healthcare sector is sparse, highlighting a significant gap in the understanding of the full scope of their contributions. This gap includes the lack of comprehensive stakeholder analysis within healthcare cooperatives, which is essential for assessing their impact and sustainability. While some studies have explored stakeholder management in private and public healthcare settings (see San-Jose et al., 2021; Molinero et al., 2021), there is a noticeable lack of focus on healthcare cooperatives (see Pereno & Eriksson, 2020; Thadani, & Patnaik, 2023).
This study employs a qualitative case study methodology to explore the Moncloa University HLA hospital, a health cooperative, using stakeholder theory and the SPOLY methodology (Ayuso et al., 2020; Freeman et al., 2020; Retolaza et al., 2016; San-Jose & Retolaza, 2016). The SPOLY methodology helps differentiate between market and non-market social value, providing a robust framework for analysing stakeholder contributions. Data collection involves extensive document review, interviews with key stakeholders, and analysis of secondary sources to construct a detailed stakeholder map.
By focusing on Moncloa University HLA Hospital, this research seeks to address the gap in the existing literature on the management of stakeholders and value creation in healthcare cooperatives. The aim of this paper is to show the stakeholder map of a healthcare cooperative, highlighting the interactions and contributions of each stakeholder group, and demonstrating how these relationships foster value creation, enhance sustainability, and address long-term challenges within the healthcare sector. The study provides empirical evidence of the benefits and challenges associated with cooperative healthcare models, offering insights into their role in enhancing healthcare sustainability and addressing long-term sector challenges. The findings indicate that healthcare cooperatives operate at the intersection of public and private healthcare models, driven by cooperative values that prioritize stakeholder engagement and value creation, rather than profit.
The structure of this paper is as follows: the introduction outlines the context, relevance, research problem, methodology, contributions, and structure of the study; the theoretical framework discusses stakeholder theory and its application in the healthcare sector, emphasizing the role of cooperatives; the methodology details the qualitative approach, data collection methods, and analysis techniques used in the study; the case study analysis presents the findings from the Moncloa University HLA Hospital case study, including the identification of stakeholders and the value generated for each group; the discussion analyses the implications of the findings, comparing them with existing literature and highlighting the unique contributions of healthcare cooperatives; and the conclusion summarizes the key findings, discusses the limitations of the study, and suggests directions for future research.
2.1. The health system from a stakeholder view
Health is widely recognized as one of the fundamental pillars of the welfare state, playing a crucial role in improving individuals' quality of life and contributing to the overall well-being of society (McKee & Healy, 2002; Navarro, 2004). However, health systems today face a multitude of complex challenges that threaten their long-term sustainability. These challenges include climate change (WHO, 2022), population aging (Moreno Sanchez, 2019; Riesgo, 2007), the management of limited resources and justice issues (Lamata, 2020; Sandel, 2011; Buitrago Peña & Gómez Toro, 2021; Comité de Bioética de España, 2016; de la Torre, 2017, 2020; Lecaros Urzúa, 2016; Rendtorff, 2015), the inclusion of ethics and consideration of vulnerable populations (Buitrago Peña & Gómez Toro, 2021; Comité de Bioética de España, 2016; de la Torre, 2017, 2020; Lecaros Urzúa, 2016; Rendtorff, 2015), stakeholder involvement in decision-making (Freeman, 1984), technological integration and disruption (Feito, 2019), and the influence of social determinants of health (Gil et al., 2015).
These issues extend far beyond the healthcare systems themselves, impacting society at large and highlighting the need for a comprehensive approach to health policy. By addressing these challenges, health systems not only ensure their own sustainability, but also create significant value for society by enhancing overall social well-being, fostering economic stability, and contributing to the development of healthier, more resilient communities (Kroeger & Weber, 2014; Pereno & Eriksson, 2020; Thadani & Patnaik, 2023).
In healthcare, the hospital serves as the central structure for managing conflict resolution, challenges, and tasks, making it a critical unit of analysis for value generation. Previous studies have focused their work on this area, but there is a gap in the co-operative health sector which has not yet been addressed but which undoubtedly has great repercussions, since the great value of the co-operative system undoubtedly lies in the worker, who is the executor, strategist and facilitator of the hospital's day-to-day operations. The co-operative system also allows not only governance based on generating value for the employee, but also co-operative values ensure that such value is passed on in the form of a legacy to future generations.
Consequently, it is essential in healthcare to include both workers and other stakeholders in the core of governance to generate value efficiently. Malfait et al. (2017), for example, highlight improvements in hospital business processes through diverse stakeholder inclusion in decision-making, optimizing both efficiency and operational effectiveness. Similarly, Tampio et al. (2022) underline the importance of stakeholder analysis in hospital project planning and execution, indicating that a thorough understanding of stakeholder relationships can lead to more meaningful and sustainable value creation. Nandraj et al. (2001) address hospital accreditation in India, suggesting that a stakeholder-inclusive approach can lead to more relevant and comprehensive accreditation standards, improving the quality of health services. García-Armesto et al. (2010) evaluate Spain's healthcare system, highlighting how the organization, financing, and management impact service delivery and patient outcomes. Casasnovas et al. (2009) examine the effects of decentralization on managerial autonomy within the Catalan hospital sector, which may positively influence healthcare efficiency and delivery.
In summary, these studies emphasize the need for adaptive and collaborative management in the health sector, incorporating decentralization and active stakeholder participation to improve health systems.
2.2. The role of stakeholder theory and social accounting in sustainable healthcare
Freeman's (1984) foundation of stakeholder theory emphasizes the importance of addressing the interests of all stakeholders in strategic management. By creating value for customers, suppliers, employees, communities, and financiers, organizations can achieve long-term success. In the case of cooperative hospitals, this involves engaging with a diverse range of stakeholders to understand their needs, thereby enhancing patient care and community well-being.
Harrison et al. (2010) built on Freeman’s work, demonstrating that managing for stakeholders, rather than solely for shareholders, leads to better organizational outcomes and sustainable competitive advantage. This approach is especially relevant for cooperative hospitals, which must balance financial performance with social objectives. A stakeholder-focused approach improves operational efficiency, patient satisfaction, and community ties, leading to more sustainable healthcare services.
San Sebastián & Barandiaran (2022) and San-Jose et al. (2017, 2021) highlight the importance of social accounting in healthcare, particularly for cooperative hospitals. They emphasize internal collaboration across departments to identify and quantify social value, ensuring alignment with the hospital's mission and stakeholders' needs. These models facilitate better strategic decision-making and transparent reporting of social impacts.
Mendizabal and Garcia-Merino (2020) explored the social value in sports clubs, noting the significance of emotional value in stakeholder relationships. Pereno & Eriksson (2020) and Thadani & Patnaik (2023) further discussed sustainable business practices and the role of social accounting in corporate governance, advocating for robust methods to capture and report social value in business operations.
Collectively, these contributions underscore the evolving landscape of social accounting and stakeholder theory, advocating for inclusive and comprehensive approaches to value measurement and reporting in cooperative and socially-oriented organizations.
Thadani & Patnaik (2023) address the challenges and limitations of the public and private healthcare systems in developing countries. They propose a conceptual framework for sustainable healthcare cooperatives based on the Spanish model, incorporating cooperative worker insurance to provide affordable, high-quality health services. This model ensures that all income brackets, including the low-income population, receive timely and good-quality health services at an affordable price, empowering individuals to invest small amounts as premiums for a healthier future.
2.3. The cooperative Hospital as a value generator in the social economy
The debate focuses not only on the hospital as a generator of value but more specifically on the co-operative hospital as a generator of value for society and stakeholders.
It is important to note that the social economy has significant economic relevance in Spain, contributing an estimated 8% of GDP and accounting for more than 2 million jobs, which is 12.5% of total employment (CEPES, 2022). In healthcare, doctor cooperatives generate around 35,000 jobs and have a turnover of approximately 1.5 billion euros (CEPES, 2022; Government of Spain, 2022).
Social economy organisations, such as the Espriu Foundation, define a model of social medicine based on dialogue in the doctor-patient relationship. The aim is to enhance the social value of health care and human capital through cooperativism. Management is co-responsible between users and professionals, without intermediaries, and profits are reinvested in the quality of care (Espriu Foundation, 2024).
According to the Espriu Foundation and the Spanish business confederation of the social economy (CEPES) (2018), society must be aware of the social medicine model, as it facilitates citizens' access to healthcare, improves conditions for medical practice, and consolidates the sustainability of the healthcare system. The co-operative health care model serves more than 2.5 million patients annually (CEPES, 2018).
Dr. Zarco states that "health care in the framework of the social economy is a third way between public and private health care“. This model's primary objective is to offer quality, accessible care, making it a compelling study to determine how health co-operativism can address the public/private health care dichotomy (Zarco, 2018).
Similarly, Dalwai et al. (2023) discuss how health co-operatives are emerging as viable and sustainable solutions to health service provision challenges. They examine global experiences and provide recommendations for the future development of these co-operatives, stressing that they not only provide accessible medical services but also promote self-management and community responsibility in health care.
On the other hand, Duffy and Oemichen (2005) explore how co-operative principles can improve the value and quality of health services. They argue that health care co-operatives can effectively integrate the values of equity, mutuality, and accountability into the health care system, offering a patient-centred alternative to commercial health care models. These authors emphasize the importance of a co-operative structure in enhancing the care and satisfaction of both patients and health care providers.
Thus, there is a need to present the stakeholder map of a hospital with social characteristics and the value that can be derived from these relationships due to their alignment with achieving value for all parties involved. This approach will not only contribute to the existing literature, such as the work by Tampio et al. (2022), but also provide insights into value generation from a social economy perspective.
An exhaustive analysis of the situation is required to conduct this study, which is why it is not possible to carry out sample or statistical analyses or to test hypotheses, as we are still at an incipient stage of generating propositions. In this way, case analysis is the most suitable methodology, as it allows us to understand the context and the reality of a unit of analysis as a whole. In this case, following the proposals of Yin (2009) and Stake (2005) together with the framework of reference proposed by Freeman (1984) in their understanding of stakeholders, we will be able to answer the questions raised in this paper.
The definition of stakeholders is based on a qualitative methodology. This methodology aims to generate a theoretical framework based on observation and data (Moghaddam, 2006). (Moghaddam, 2006). In the dialogue, the dimensions are categorised and related to the literature (Grace & Lo Iacono, 2015; Sweeney & Soutar, 2001).
Stakeholder theory (Freeman, 1984) was used to construct the hospital stakeholder map. From the initial interviews and with the final purpose of providing a solid basis for the hospital's social accounting process. The stakeholders of the specific organisation, in this case those of Moncloa University HLA Hospital, must be identified; as well as the perceptions that these stakeholders have about the value received by their organisation, and subsequently, the non-market value associated with these perceptions must be calculated.
The SPOLY methodology, which helps to understand and differentiate between market and non-market social value, is used as the basis for the analysis (Retolaza, 2022; Retolaza & San-Jose, 2016). The SPOLY methodology has been used in the literature (Arimany-Serrat & Tarrats-Pons, 2021; Ayuso et al., 2020; Barba Sanchez et al., 2021a, 2021b; Barba-Sánchez et al., 2021; Etxezarreta-Etxarri et al., 2018; Guzmán Pérez et al., 2020; San-Jose et al., 2021) to reflect the social value, facilitating the interpretation and discussion of results. It is based on stakeholder theory and is structured in six phases (Retolaza et al., 2015; San-Jose & Retolaza, 2016). Along these lines, other authors such as Ayuso (2023) and Aguado et al. (2021) have also applied it to the social economy; the former to special employment centres and the latter to a system of multiplier development within foundations.
It is worth making a methodological mention of what is understood as social market value and social non-market value (Retolaza et al., 2015). The social market value is the one obtained from market transactions. It is therefore extracted from financial information. Non-market value is understood as the non-economic value that the company brings to its stakeholders and that is not reflected in financial information or market transactions (Economic Alternatives, 2022).
As regards the unit of analysis, these are the reasons why this hospital has been considered suitable.
Firstly, this hospital is suitable for a case analysis because of its particular size, being a medium-large size among those with healthcare capacity. Secondly, it is a hospital of its own hospital group, among those that are well endowed, which ensures that its activities are focused on achieving value for society, and thus for its stakeholders. Thirdly, its controlled extrapolation and comparison with other hospitals with similar characteristics can follow the analysis. Finally, from a more practical perspective, the proximity of the management, their transparency and dedication to the project allow for an exhaustive analysis; this qualitative analysis can therefore be carried out with precision.
In addition, the following table (see Table 1) shows the main characteristics of the hospital:
Table 1. Descriptive variables of the unit of analysis.
|
Variable |
Datum |
|
Hospital Name |
Moncloa University HLA Hospital |
|
Size |
28,000 m2 distributed over four floors. 218 single rooms with a companion bed 7 premium suites 12 suites with lounge 13 I.C.U. posts 14 operating theatres for high surgery (2 ophthalmological) 1 delivery room 60 specialised care areas and units 43 specialist consultations |
|
Constitution Year |
1993 |
|
Location |
Madrid (Spain) |
|
Web |
HLA Hospitals |
|
Dependence on |
Lavinia S. Coop |
|
Owner |
ASISA-LAVINIA S. COOP. |
|
Certifications |
ISO 9001, ISO 14001, Excellence, SG21 Forética, Ambassador of European Excellence, QH3, EFQM |
|
Care data 2022 |
Consultations: more than 170,000 Diagnostic imaging tests: over 80,000 Laboratory determinations: 3 million Emergencies: more than 50,000 Interventions: more than 21,000 |
Source: own elaboration.
The group has a healthcare model based on excellence, innovation, quality care and a human and close relationship with the patient. It is non-profit and reinvests its profits in the improvement of its human and technological equipment, the modernisation of its facilities and the training of its professionals. Moncloa University HLA Hospital was built in 1993. It is part of the HLA network of hospitals, integrated within the ASISA Group of companies dependent on Lavinia S. Coop., the largest medical co-operative in Spain and Europe. It is made up of more than 9,000 doctors. It is the centre with the largest healthcare capacity in the hospital group. The group is one of the largest hospital providers in Spain, with more than 40 years of experience. It is made up of 18 hospitals and 35 multi-specialty centres with reference units and state-of-the-art treatments. It has 1,300 beds, working in an integrated way to offer access to high quality healthcare.
Located in Madrid (Spain), the Moncloa University HLA Hospital was built in 1993 and has a surface area of 28,000 m2 distributed over four floors. It has 218 single rooms with a companion bed, 7 premium suites, 12 suites with lounge, 13 ICU stations, 14 operating theatres for major surgery (2 ophthalmology), 1 delivery room, 60 specialised care areas and units, 43 speciality consulting rooms, a post-surgical resuscitation unit, a nest, a sterilisation centre and a complete day hospital. During the year 2022, the hospital obtained the following healthcare data:
· Consultations: more than 170,000 (8% more than in 2021).
· Diagnostic imaging tests: more than 80,000 (5% more than in 2021).
· Laboratory determinations: almost 3 million (7% more than in 2021).
· Emergencies: more than 50,000 (9% more than in 2021).
· Interventions: more than 21,000 (13% more than in 2021).
The hospital has been included in different lists and indicators of reputation and quality, as have some of its specialities. It also has the Madrid Excellent recognition, awarded by the Community of Madrid. It also boasts several certifications such as Q for quality, the FACE Gluten Free agreement or standards such as SEG21 from Forética or ISO 9001, 14001 and 45001. Below is a list of the certifications held by the hospital:
· Recognition from Madrid Excelente
· ISO 9001 Certification
· European University
· ISO 14001 Certification
· European Seal of Excellence (600+)
· ISO 45001 Certification
· Forética's SG 21 Certification
· Global Pact (United Nations)
· ICTE Certification. Health tourism
· "Ambassador of European Excellence" (by the High Commissioner for Marca España)
· QH 3-star accreditation by the Institute for the Development of Health (IDIS)
· Recognition of excellence: ICTE's Health Tourism Quality Standard.
· National Award for Excellent, Innovative and Sustainable Management in the Large Organisation Category for outstanding management and commitment to the EFQM model.
· 10th place nationally in the ranking of the Health Reputation Monitor (MRS).
In order to carry out the analysis, the documentation and reports, websites and official accounts were exhaustively reviewed. The analysis was completed by conducting interviews, in various stages, based on the stakeholders identified in the search for variables of value. Thirty-nine interviews were conducted, totalling 975 minutes. The following table shows the main characteristics of the interviews conducted.
Table 2. Characteristics of the interviews conducted at the hospital.
|
Stakeholder |
Number |
Online/Online (%) |
Recording (%) |
Transcription (%) |
|
Suppliers |
6 |
33 % on-site 67 % online |
100% |
100% |
|
Workers (3 groups) |
20 |
70 % face-to-face 30 % online |
100% |
100% |
|
Patients |
5 |
100 % face-to-face |
100% |
100% |
|
Civil society organisations |
1 |
100 % online |
100% |
100% |
|
Cooperativists |
5 |
20 % online 80 % face-to-face |
100% |
100% |
|
Group companies |
2 |
50 % face-to-face 50 % online |
100% |
100% |
Source: own elaboration.
The researcher who conducted the interviews was objective at all times; although there is always a certain bias and involvement as interviewer and result analyst, we have established a plan to reduce this bias, by contrasting the results with two other researchers in such a way that the conclusions were only considered to be correct when the same conclusions about the interviews conducted were reached.
4.1. The case of the Health System in Spain and the link with bioethics committee's perspective
Although this is a classic problem, it is still a topical one. There is no common model in the Spanish Health System that compares the efficiency of the different Health Services managed by the different Autonomous Communities (Sabando & Rey del Castillo, 2020), nor a model that allows the comparison of efficiency between hospitals within the public network (Pérez-Romero et al., 2017) or in private hospitals.
These challenges have a direct impact on people and their vulnerability. It is not beneficial to view sustainability in health systems from a single perspective. (Spanish Bioethics Committee, 2016, but it is advisable to approach them from a multidisciplinary perspective. Sustainability therefore needs to be approached from a vision that goes beyond economic management.
In the case of Spain, in 2016 the Spanish Bioethics Committee (CBE) issued the Ethics and responsibility in the sustainability of the national health system with the intention of contributing to public reflection on the sustainability of the public health system in Spain declaration. (Spanish Bioethics Committee, 2016). Along with representatives from the autonomous regions, the CBE calls for consensus on the sustainability of the National Health System (NHS) in order to preserve its quality of care and its social role within the welfare state.
The CBE refers to both the ethical and legal basis mandated by the Constitution. It calls for alignment with the general interest and common good, ensuring continuity and evaluation of projects. The CBE also highlights the co-responsibility of various agents in NHS sustainability: healthcare professionals, managers, politicians, media providers, and citizens (Spanish Bioethics Committee, 2016). The issue of stakeholders underpins a case study on healthcare systems and centres. Annex 1 displays the level of co-responsibility of different agents in NHS sustainability according to the CBE. Stakeholders in healthcare bear broad, interconnected, and significant responsibilities. Healthcare professionals are key decision-makers who influence criteria affecting people's well-being. Politicians can tighten the system, impacting risks based on resource allocation decisions. These decisions directly affect the welfare of citizens and patients.
It should also be noted that the CBE reaches four conclusions in this document that are the pillars for healthcare in Spain, and which will undoubtedly condition the generation of value of any hospital in the national healthcare system. (Spanish Bioethics Committee, 2016):
1. Firstly, society aspires to a public, universal, quality and solidarity-based NHS, for which it is essential to achieve its sustainability.
2. Adequate funding is not a sine qua non.
3. Responsibility is shared by all agents involved in the efficient functioning of the NHS, which should lead to a process of reflection that opens up new horizons and perspectives.
4. Finally, based on the declaration's ethic of responsibility, it is proposed to open a social debate that will help to adopt concrete initiatives and measures that can be evaluated in the areas involved in the sustainability of the NHS.
On the basis of this statement, it can be affirmed that the sustainability of the NHS in Spain requires the inclusion of ethics in healthcare management, while integrating the interested parties. Therefore, the problem of sustainability is not exclusively economic. It is necessary to seek new reference frameworks based on stakeholders that allow initiatives and specific measures to be measured and evaluated responsibly. With regard to co-responsibility and ethics in health management, there is ample mention in the literature providing perspectives at micro, macro and meso levels (Geels, 2002).
4.2. The case of Moncloa University HLA Hospital
With the methodological process described above, the different stakeholders are identified in order to draw up a first map of stakeholders in which the main areas are taken into account.
The literature on stakeholder identification (Freeman, 1984; Harrison et al., 2010; Mendizabal et al., 2020; Molinero et al., 2021; San Sebastián & Barandiaran, 2022; San-Jose et al., 2017, 2021) provides insights into the organisation’s explicit knowledge, mission, strategy, values, and culture. Considering the recent past (Retolaza, 2022; San Sebastián & Barandiaran, 2022), various internal working groups were formed. These included different hospital departments such as the Medical Directorate, Management, Human Resources, and Sustainability. A review of internal documents and processes allowed for an initial approximation of the hospital's stakeholder map (see Figure 1).
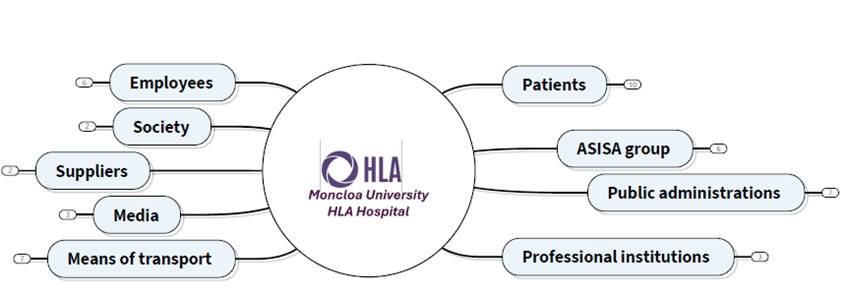
Figure 1. Provisional stakeholder map of Moncloa University HLA Hospital (HLA Hospital Universitario Moncloa). Source: own elaboration.
Due to the very nature of the co-operative nature and the healthcare activity of the group of companies, human capital is a major asset for the performance of the activity and a strategic pillar for the hospital. The healthcare sector is hardly conceivable without the professionals that make it up, with a multitude of links such as the doctor-patient relationship or the care relationship (de la Torre, 2017; Ferrer & Álvarez, 2003; Gracia, 2008; Roqué-Sánchez & Gonzalvo-Cirac, 2015).
The hospital's corporate culture takes into account quality of care (Espriu Foundation, 2024) as it connects the corporate values, the company's vision and mission, and the doctor-patient relationship. In this regard, it should also be noted that the nature of the organisation promotes and enhances the quality of care. This stakeholder groups together all the hospital's employees.
Today's competitive environments suffer from great volatility in global and local terms. Due to the challenges faced by societies, it is necessary to propose a vision of co-responsibility that can be embraced by the whole of society and the search for references that will improve the system. In such a complex and highly regulated sector as health , social demands must be taken into account in order to build more responsible and sustainable environments. Social conditions and contexts determine people's health, which is why the hospital context must mitigate these differences in order to benefit society as a whole. In addition to other currents around single health that fall under the umbrella of the One Health concept, which aligns with the SDGs to address issues such as dignity, peace, and prosperity for people and planet now and in the future, this study also aims to show the relationship between stakeholder management and value generation in healthcare cooperatives. The term is proposed during the early years of the 21st century as a multidisciplinary approach with the joint and simultaneous work of several disciplines that has revolutionised the concept of health and its relationship with sustainability. As happens on many occasions, when the concept is investigated we realise that it is not so current. Already in antiquity, Hippocrates had a vision of the association between a clean environment and health. During the Renaissance or the 19th century, the collaboration of different disciplines or a holistic approach to the arts were proposals advocated by Da Vinci, Pasteur or Koch among others. More recently, in the middle of the 20th century, Schwabe conceptualised in "one medicine" a concept very similar to One Health as the interrelationship between human and animal health and their relationship with the surrounding environment. (Barton Behravesh, 2019a; Ruiz, 2018).
In this vision of generating value for stakeholders, reference has been made to society and special importance has been given to communities or cities that have a direct relationship with the hospital or are of special strategic interest to the Group. Furthermore, suppliers and creditors have been included as an important stakeholder, due to their fundamental role in the organisation's activity. This is evident in the argument used by supplier so-codified S1 that literally states "Maintaining a relationship with HLA allows us to generate stable and quality employment. We have the security offered by a solid entity with cooperative values that maintains stable relationships over time and allows us to grow together". This has been taken into account, as the company's reflections argue that many of the company's activities depend on global value chains, in which it is difficult to know the real social impact of the activities without taking into account the companies that depend on the different operational areas of the group and specifically of the hospital. Similarly, the inclusion of suppliers in the strategic and sustainability thinking is essential in the search for fair sustainable development for all parties, as can be seen from the various documents on corporate sustainability of the European Union.
Social networks and the media play an important role in terms of information in society in general and in healthcare in particular. The responsibility that this stakeholder has in reference to the healthcare system or the healthcare sector has been echoed by different institutions such as the Spanish bioethics committee, public institutions or the collegiate bodies representing healthcare professionals in Spain. This idea can be perceived in the statement given by the interviewees: "They are fundamental for communicating issues to do with people's health (and the concept of health). They are also fundamental for the social economy because they help citizens to learn about its activities". Moreover, as a consequence of the pandemic, the process of digital transformation in healthcare companies has been boosted by tools for communicating with patients, managing appointments and waiting lists, and the progressive inclusion of artificial intelligence and computer applications in healthcare processes. Although they have developed most strongly around the management derived from healthcare. For the above reasons, the cataloguing of a media stakeholder has been taken into consideration.
As the Moncloa University HLA Hospital is, as mentioned above, a hospital belonging to the HLA Group and in turn dependent on ASISA, a specific stakeholder has been included in which all ASISA Group companies are taken into account. The hospital is a point of reference for many people and thousands of co-operative members throughout Spain. Strategically, it generates shared value with the other companies, as it helps to provide the insured and patient alike with a comprehensive range of care, in which the hospital is a key player. This idea was expressed by at least one of the interviewees, who pointed out that "for the Group to have its own hospitals with which it shares a common purpose and co-operative values generates a differential value. Between the different healthcare and insurance activities we bring to society a unique project".
However, stakeholder patients include all those people who have some kind of healthcare relationship with the hospital. These patients may be insured by ASISA, other insurance companies, state mutual insurance companies, the National Health System or private insurance companies. The patient, who is strategically at the centre of the hospital's activities, is of paramount importance in the identification of the stakeholders of Moncloa University HLA Hospital. This idea can be aligned with what one of the patients interviewed stated: "The treatment we receive at the hospital generates a great deal of peace of mind. Something that generates a lot of value is the level of quality of care and humanity received at the hospital. Knowing that you are in good hands. The reinvestment of profits is seen in the continuous improvement of the facilities". Please refer to Annex 2 for a summary table detailing the value perceived by patients regarding the hospital's services.
In Spain, the healthcare activity and the range of services offered by healthcare centres is strictly regulated by the public administrations. Specifically, these powers are today held by the Autonomous Communities and the Ministry of Health. The hospital's healthcare activity is therefore subject to these institutions. Making them a key stakeholder in the hospital's healthcare activity, an idea that is expressed in the following statement made by one of the interviewees: "The function of the hospital, which complements the National Health System, generates value for me. It also improves the health of the citizens and this has repercussions for the public administration". Undoubtedly, a reciprocal value generated.
The stakeholder of professional institutions groups together the associations and collegiate bodies of the professionals working at Moncloa University HLA Hospital. This stakeholder also includes the training centres (vocational education and training centres and universities) which are key to the training and qualification of healthcare staff. Finally, it also takes into consideration the associations and organisations in the health sector.
A stakeholder called means of transport is identified to conclude the first approximation of the stakeholder map at Moncloa University HLA Hospital. This takes public transport, taxi services and chauffeur-driven vehicles into account, as well as companies dedicated to the rental of electric scooters, bicycles and vehicles. With regard to transport, it has been pointed out that "they are fundamental and generate a lot of value. Many people would not be able to come to the hospital if it were not for public transport services. In addition, their use by patients contributes to the environment".
Once the first stakeholder map of Moncloa University HLA Hospital has been defined, work begins on deepening and seeking consensus through dialogue with management and the different management areas. This work is carried out taking into account the feedback received by the experts. Through this process, as described above, the methodology aims to build a stakeholder map that reflects in depth the areas described from the perspective of the generation and impact of social value. There are two issues to highlight in the definition of the stakeholder map. Firstly, the strategic vision of the hospital must be taken into account when constructing the map and contextualising it so that it is relevant to hospital management. This approach contributes to the identification of stakeholders who have an impact on the sustainability of the healthcare system according to the Spanish Bioethics Committee, and thus helps to translate technical and bioethical deliberations into management. The following figure (see Figure 2) shows the result using the agreed stakeholder map of the HLA Moncloa University Hospital.
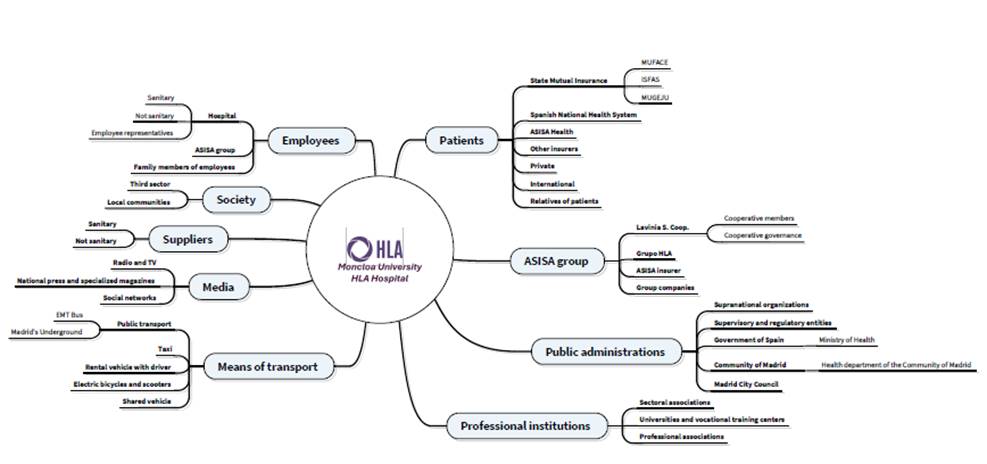
Figure 2. Stakeholder consensus map of Moncloa University HLA Hospital. Source: own elaboration.
As a co-operative, the figure of the worker is of particular importance, which is why the definition of the worker was developed in collaboration with the Human Resources Department. It is worth mentioning that three different versions of this definition emerged, and it was even proposed that this stakeholder be defined taking into account the vertical and horizontal structure of the hospital itself. The following stakeholders of the employee group were taken into account in this draft: management, middle management, doctors, other healthcare staff, administration and management, trade unions and family members. Difficulties soon arose in drawing up the map. When the outline of this type of structure was drawn up, there was a dispersion of the different stakeholders. It created difficulties to interpret the methodological process and could be further schematised without losing the representation of any of these stakeholders, being in line with the literature (Harrison et al., 2010; Mendizabal et al., 2020; San Sebastián & Barandiaran, 2022).
During the methodological process, and as a result of the dialogue arising from the need to integrate the different positions of the hospital's human capital structure, a response to the problem described above emerged. Three subgroups were created in which the different professional categories were taken into account. The first subgroup refers to the hospital's employees, which in turn are divided into healthcare staff and non-healthcare staff and employee representatives. Healthcare staff refers to all those healthcare professions that have a direct relationship with the patient or with the care processes. Non-health staff refers to workers who have administrative and managerial functions. Workers' representatives and trade unions are included in the hospital as they are directly involved in the hospital's activities. They are not taken into account from a business group perspective, as labour relations are carried out by healthcare workplaces and not by other activities of the group companies.
The second subgroup is called the ASISA Group and refers to the Group's employees who have some connection with the hospital's activities as a result of the synergies arising from the activities of the various companies within the Group. Finally, the subgroup of family members is added, which takes into account the relatives of hospital employees, as many measures or decisions taken by Human Resources indirectly influence the relatives of employees. In this sense, work-life balance, social benefits, training and promotion, etc.measures can be highlighted.
The society as a whole is represented in a stakeholder shaped through collaborative work and has been defined in internal deliberation processes (Mendizabal et al., 2020). It is a fairly generic stakeholder that encompasses society as a whole. Its perspective can be assumed from the very community in which the hospital provides its healthcare service or even, when understanding society from a much broader perspective, it can be encompassed by currents close to the OneHealth concept (Barton Behravesh, 2019b; Ruiz, 2018). The third sector, in the health context, assumes a relevant role. The organisations and associations that make it up and constitute the social economy cannot go unnoticed by companies (even more so in the case of a health cooperative). A differentiation is made around the communities in which the hospital has a healthcare activity, as well as the sectoral associations directly related to this activity.
The development of the supplier stakeholder has been carried out in coordination with the operations management and the hospital management. The smooth running and logistics of the hospital depend to a large extent on this area, which is why it is considered strategic. This, in turn, is divided into two subgroups: care and non-care.
Suppliers are those directly related to healthcare activities: pharmacists, doctors (healthcare professionals) or healthcare products and services. Non-care providers include other suppliers such as general services, advisory and consultancy services, maintenance services and technology.
In the media, national and regional radio and television are taken into account. The national press and specialised magazines are also considered relevant. The digital environment is considered relevant after the irruption of social networks, which are also included in this stakeholder group. The current world cannot be understood without the media and social networks; their role is indispensable in the conceptual understanding of health and health activities.
The stakeholder group of the ASISA Group is subdivided into four notable groups. Firstly, the Lavinia co-operative, which owns the hospital. In turn, its partners and governing bodies are taken into account. Secondly, it takes into account the healthcare network of which the hospital forms part (HLA group), fourthly, it takes into account ASISA as a health insurer and thirdly, the other companies that make up the group and which carry out different healthcare activities (ophthalmology and dental clinics, clinical analysis laboratories, assisted reproduction units, etc.).
Due to the hospital's culture, principles and values, the stakeholder patient is given close attention. It has been divided into the following subgroups (of course, there is no differentiation in the treatment of patients on the basis of their origin; these are merely descriptive categories):
· Patients coming from the three State mutual insurance companies: Mutualidad General de Funcionarios Civiles del Estado (MUFACE), Instituto Social de las Fuerzas Armadas (ISFAS) and Mutualidad General Judicial (MUGEJU).
· Patients referred from the National Health System (NHS)
· Patients with ASISA Health insurance.
· Patients with health insurance from other insurers.
· Private patients.
· International patients.
· Relatives of patients.
Public administrations, including the public bodies that regulate and supervise healthcare activity, as well as supranational organisations, the central government, the Community of Madrid and the Madrid City Council, are relevant to the hospital's activity.
Professional institutions are mentioned as a stakeholder, and there is collaboration with business or sectoral associations in meeting forums to learn about trends and innovations in areas of interest to the hospital. In order to attract talent or research, including a subgroup of universities and training centres is deemed to be necessary. Professional associations are considered important for the hospital's own activity and for the promotion of sectoral and professional dialogue.
Finally, the means of transport is considered a relevant stakeholder due to the hospital being located in a large city. This includes traditional means of public transport such as taxis, buses and the metro, as well as the new sustainable mobility options that have emerged in cities: bicycles and electric scooters, car sharing and chauffeur-driven transport vehicles.
Molinero et al. (2021) developed a stakeholder map for the Santa Marina Hospital in Bilbao with fewer stakeholders. The key differences in this study are: firstly, the type of management, as Santa Marina Hospital belongs to the Basque Health Service, whereas Moncloa University HLA Hospital is a cooperative hospital. One is integrated into the public health system, while the other, although collaborating with it, serves state mutual insurance companies and private health patients. Secondly, cooperativism seems to affect the number and type of stakeholders. Although both hospitals share common groups such as patients, workers, public administrations, and professional institutions (e.g., medical colleges and students), the cooperative group is unique to Moncloa University HLA Hospital. This group's importance lies in being the hospital's ultimate owners, positioning the hospital between public and private realms, driven by cooperative values where profit is not the primary objective. Therefore, this study aims to show the relationship between stakeholder management and value generation in healthcare cooperatives.
This study explores the role and impact of healthcare cooperatives in generating value for stakeholders, using the Moncloa University HLA Hospital as a case study. These findings show that healthcare cooperatives bridge the gap between public and private healthcare models, offering efficiency, accessibility, and stakeholder engagement. By prioritising cooperative values over profit, the organisations support the sustainability of the healthcare system, especially the Spanish National Health System.
The study makes a theoretical contribution in line with stakeholder theory, and it refers to developping a nine-group stakeholder map: workers, society, suppliers, media, the ASISA group, patients, public administrations, professional institutions, and transportation services. The relevance lies not only in the number of stakeholders but also in their types, as they influence the results, strategies, and operations of healthcare cooperatives. Stakeholders are key in decision-making in both public and private hospitals. There are few studies analysing stakeholder groups in the healthcare system, both in Spain and internationally. Therefore, this study fills a significant gap in the literature, providing a comprehensive understanding of the diverse and interconnected roles that stakeholders play in the healthcare sector. This enhanced perspective aids in formulating strategies that can leverage stakeholder engagement for improved healthcare outcomes and system sustainability.
However, the most relevant practical implications refers to a new approach for analysing the efficiency of the health system, based on the ratios generated by dividing the outputs generated by the inputs used. The use of social accounting makes it possible for both outputs and inputs to be expressed in monetary units without the need for qualitative analysis. Secondly, although incipient, this article opens up a field of research that goes beyond the individual case to allow macro analyses of the health services of a given country or territory.
Consequently, the practical recommendations are the following ones. First, hospital managers should prioritize patient-centred care by enhancing access to qualified professionals, expanding emergency services, and implementing digital health tools, such as medical chat and video consultations. Focusing on specialized units and sustainability initiatives will further align hospital services with patient values, fostering trust, efficiency, and overall well-being. Second, this new perspective facilitates the objective analysis of the complementarity between the different types of capitalist, social and public health care, meaning that the efficiency of each of the organizational structures can be identified in relation to the different stakeholders and the different areas of value transfer in a cross-cutting manner.
The study's primary limitation is its reliance on a single case study, which may not fully capture the diversity of experiences and impacts across different healthcare cooperatives. The qualitative nature of the research, while providing deep insights, limits the generalizability of the findings. Additionally, the study was constrained by the availability of data and the willingness of stakeholders to participate in interviews, which may have introduced biases. Another constraint is the focus on the Moncloa University HLA Hospital, which is relatively large and well-established. Smaller or less established cooperatives might face different challenges and opportunities, which this study does not address. The dynamic and evolving nature of healthcare systems also means that the findings may need to be revisited in light of future developments and policy changes.
Future research should aim to address these limitations by including a larger sample of healthcare cooperatives from diverse geographical and organisational contexts. Comparative studies between different types of cooperatives and traditional healthcare models would provide a more comprehensive understanding of the relative benefits and challenges. Quantitative research methods, such as surveys and statistical analysis, could complement the qualitative insights gained from this study, offering a broader perspective on the impacts of healthcare cooperatives. Longitudinal studies would also be valuable in assessing the long-term sustainability and effectiveness of cooperative models in healthcare.
Overall, this study underscores the potential of healthcare cooperatives to significantly enhance the sustainability and effectiveness of healthcare systems. The Moncloa University HLA Hospital exemplifies how cooperative values can drive positive outcomes for a diverse array of stakeholders, including patients, employees, public administrations, and suppliers. Its unique cooperative structure, encompassing stakeholders such as the ASISA group and transportation services, illustrates how these organizations can create value beyond traditional healthcare models. Continued research in this area is crucial to fully understand and leverage this potential, ultimately improving healthcare outcomes for all stakeholders involved.
There is no conflict of interest.
The conceptualization, investigation, and funding acquisition were shared responsibilities of authors. Aut1 contributed significantly to data curation, formal analysis, and validation. Aut2 was instrumental in methodology, project administration, and resource management. Aut3 played a key role in software development, visualization, and writing – both the original draft and review & editing.
We are deeply grateful to the editor and reviewers for their work.
Funding
This research is being carried out within the ECRI group at UPV/EHU (GIU22/003) and FESIDE (BOPV24) as part of grants for industrial thesis projects.
Aguado Muñoz, R.; Retolaza Ávalos, J.L.; Alcañiz González, L. (2021) Social accounting in organizations of the Social Economy: The ARTE program applied to the CLADE Group. REVESCO. Revista de Estudios Cooperativos, vol. 138, e73865. https://dx.doi.org/10.5209/reve.73865.
Ayuso Siart, S. (2023). El valor social generado por los centros especiales de empleo en España: comparación de dos enfoques de monetización. REVESCO. Revista de Estudios Cooperativos, 1(145), e91411. https://dx.doi.org/10.5209/reve.91411.
Alternativas Económicas. (2022). Manual de Contabilidad Social. Alternativas Económicas. Available at: https://alternativaseconomicas.coop/revista/extra/numero-9.
Arimany-Serrat, N., & Tarrats-Pons, E. (2021). Integrated Social Value at Universities: A Guarantee for Public Subsidies. Sustainability, 13(11), 1-13.
Ayuso, S., Sánchez, P., Retolaza, J. L., & Figueras-Maz, M. (2020). Social value analysis: the case of Pompeu Fabra University. Sustainability Accounting, Management and Policy Journal, 11(1), 233-252. https://doi.org/10.1108/SAMPJ-11-2018-0307.
Barba Sanchez, V., Salinero Martin, M. Y., & Jimenez Estevez, P. (2021a). Monetising the social value of inclusive entrepreneurship: the case of the Abono Café social economy enterprise. CIRIEC-España, Revista de Economía Pública, Social y Cooperativa, 101, 115. https://doi.org/10.7203/CIRIEC-E.101.18158.
Barba-Sánchez, V., Calderón Milán, B., Calderón Milán, M. J., & Sebastián Rivera, G. (2021b). Aproximación al valor social de un colegio rural agrupado: el caso del CRA “Sierra de Alcaraz”. CIRIEC-España, Revista de Economía Pública, Social y Cooperativa, 101, 85. https://doi.org/10.7203/CIRIEC-E.101.18098.
Barton Behravesh, C. (2019a). Introduction. One Health: over a decade of progress on the road to sustainability. Revue Scientifique et Technique de l’OIE, 38(1), 21-50. https://doi.org/10.20506/rst.38.1.2939.
Buitrago Peña, M. del P., & Gómez Toro, S. (2021). Ética para la sostenibilidad. Revista Universidad de La Salle, 1(87), 15-38. https://doi.org/10.19052/ruls.vol1.iss87.2.
Casasnovas, G. L., McDaid, D., & Costa-Font, J. (2009). Decentralization and management autonomy? Evidence from the Catalonian hospital sector in a decentralized Spain. International Public Management Review, 10(2), 103-119.
CEPES (2018). Fundación Espriu y CEPES firman un convenio para promover la Economía Social en el ámbito sanitario. https://www.cepes.es/nota-prensa/528_fundacion-espriu-cepes-firman-convenio-para-promover-economia-social-ambito-sanitario.
CEPES (2022). Los cuidados desde la Economía Social. https://www.cepes.es/files/publicaciones/137.pdf.
Comité de Bioética de España. (2016). Declaración sobre ética y responsabilidad en la sostenibilidad del sistema nacional de salud. https://comitedebioetica.isciii.es/wp-content/uploads/2023/10/declaracion_sostenibilidad_sistema_nacional_salud.pdf.
Dalwai, A., Singh, R., Khanna, V., & Rutuparna, S. (2023). The Emergence of Health Cooperatives: Experiences and Way Forward. In World Healthcare Cooperatives: Challenges and Opportunities (pp. 11-45). Emerald Publishing Limited.
De la Torre, J. (2017). Vulnerabilidad. La profundidad de un principio de la bioética. Perspectiva Teológica, 49(1), 155. https://doi.org/10.20911/21768757v49n1p155/2017.
Duffy, M., & Oemichen, B. (2005). Co-op Care: Using cooperative principals to add value to health care. WMJ: official publication of the State Medical Society of Wisconsin,104(8), 40-41.
Etxezarreta Etxarri, E., Pérez de Mendiguren Castresana, J. C., Diaz Molina, L., & Errasti Amozarrain, A. (2018). Valor social de las cooperativas sociales: aplicación del modelo poliédrico en la cooperativa para la acogida de menores Zabalduz S.Coop. CIRIEC-España, Revista de Economía Pública, Social y Cooperativa, 93, 155. https://doi.org/10.7203/CIRIEC-E.93.9953.
Feito, L. (2019). Nuevas tecnologías aplicadas a la salud. Aspectos éticos. En J. de la Torre Díaz (Ed.), Nuevas tecnologías y su impacto en la sanidad del Siglo XXI. Universidad Pontificia Comillas-Cátedra de Bioética.
Ferrer, J. J., & Álvarez, J. C. (2003). Para fundamentar la bioética. Teorías y paradigmas teóricos en la bioética contemporánea. Universidad Pontificia Comillas-Cátedra de Bioética.
Freeman, E., Retolaza, J. L., & San-Jose, L. (2020). Stakeholder Accounting: hacia un modelo ampliado de contabilidad. CIRIEC-España, Revista de Economía Pública, Social y Cooperativa, (100), 89-114.
Freeman, E. (1984). Strategic Management: A Stakeholder Approach. Pitman.
Fundación Espriu. (2024). Valores y clave del éxito. https://www.fundacionespriu.coop/es/valores-y-clave-del-exito.
García-Armesto, S., Abadía-Taira, M. B., Durán, A., Hernández-Quevedo, C., Bernal-Delgado, E., & World Health Organization. (2010). Spain: Health system review.
Geels, F. W. (2002). Technological transitions as evolutionary reconfiguration processes: a multi-level perspective and a case-study. Research Policy, 31(8-9), 1257-1274.
Gil, P., Navajas, J. F. C., Otero, J. J. G., Rodríguez, M. D., Montrull, F. B., Cabrera, R. H., & Majem, L. S. (2015). Medicina preventiva y salud pública. 12.
Gobierno de España. (2022). PERTE de Economía Social y de los Cuidados. Proyecto Estratégico para la Recuperación y Transformación Económica de Economía Social y de los Cuidados.
Grace, D., & Lo Iacono, J. (2015). Value creation: an internal customers’ perspective. Journal of Services Marketing, 29(6-7). https://doi.org/10.1108/JSM-09-2014-0311.
Gracia, D. (2008). Fundamentos de bioética (3a). Triacastela.
Guzmán Pérez, B. V., Mendoza Jiménez, J., & Pérez Monteverde, M. V. (2020). El valor social y las cofradías canarias: una aproximación a través del análisis de un caso. CIRIEC-España, Revista de Economía Pública, Social y Cooperativa, 100, 115. https://doi.org/10.7203/CIRIEC-E.100.14486.
Harrison, J. S., Bosse, D. A., & Phillips, R. A. (2010). Managing for stakeholders, stakeholder utility functions, and competitive advantage. Strategic Management Journal, 31(1), 58-74. https://doi.org/https://doi.org/10.1002/smj.801.
Kroeger, A., & Weber, C. (2014). Developing a Conceptual Framework for Comparing Social Value Creation. Academy of Management Review, 39(4), 513-540. https://doi.org/10.5465/amr.2012.0344.
Lamata, F. (2020). Financiación sanitaria: suficiencia, distribución justa y eficiencia en el gasto. En El Sistema Nacional de Salud: Pasado, presente y desafíos de futuro. Ediciones Díaz de Santos.
Lecaros Urzúa, A. (2016). Hacia una autonomía encarnada: consideraciones desde un ethos de la finitud y vulnerabilidad. Revista Latinoamericana de Bioética, 16(2), 162-187.
Malfait, S., Van Hecke, A., Hellings, J., De Bodt, G., & Eeckloo, K. (2017). The impact of stakeholder involvement in hospital policy decision-making: a study of the hospital’s business processes. Acta Clinica Belgica, 72(1), 63-71.
McKee, M., & Healy, J. (2002). Hospitals in a changing Europe (Vol. 3). Buckingham: Open University Press.
Mendizabal, X., San-Jose, L., & Garcia-Merino, J. D. (2020). Understanding and mapping stakeholders of sport clubs: particularities. Sport, Business and Management: An International Journal, 10(3), 359-378. https://doi.org/10.1108/SBM-04-2019-0029.
Moghaddam, A. (2006). Coding issues in grounded theory. Educational Research, 16(1).
Molinero, F., San-Jose, L., & Molinero, A. (2021). Valor Social Integrado (VSI) del Hospital de Santa Marina en Bilbao: monetizando el valor social para los ‘stakeholders’. Zerbitzuan, 73, 93-104. https://doi.org/10.5569/1134-7147.73.07.
Moreno Sánchez, E. (2019). Desigualdades sociales en salud. El papel de la exclusión social en el gradiente socioeconómico en la distribución de la salud y las enfermedades.
Nandraj, S., Khot, A., Menon, S., & Brugha, R. (2001). A stakeholder approach towards hospital accreditation in India. Health Policy and Planning, 70-79.
Navarro, V. (2004). El Estado de bienestar en España (pp. 15-32). Tecnos.
OMS. (2022). OMS | Constitución de la OMS: principios. WHO. Available at: https://www.who.int/home.
Pérez-Romero, C., Ortega-Díaz, M. I., Ocaña-Riola, R., & Martín-Martín, J. J. (2017). Análisis de la eficiencia técnica en los hospitales del Sistema Nacional de Salud español. Gaceta Sanitaria, 31(2), 108-115. https://doi.org/10.1016/j.gaceta.2016.10.007.
Pereno, A., & Eriksson, D. (2020). A multi-stakeholder perspective on sustainable healthcare: From 2030 onwards. Futures, 122, 102605.
Rendtorff, J. D. (2015). Case studies, ethics, philosophy, and liberal learning for the management profession. Journal of Management Education, 39(1), 36-55.
Retolaza, J. L. (2022). Marco teórico y metodológico para la monetización del valor social distribuido por los museos. En L. San-Jose & J. L. Retolaza (Eds.), Monetizando el valor social en la ecomonía naranja. El caso de los museos vascos. ESIC.
Retolaza, J. L., & San-Jose, L. (2016). Contabilidad social para la sostenibilidad: modelo y aplicación. Revista de Contabilidad y Dirección, 23, 159-178.
Retolaza, J. L., Ruiz-Roqueñi, M., & San-Jose, L. (2015). An Innovation Approach to Stakeholder Theory: Application in Spanish Transnational Corporations. Revista Brasileira de Gestao de Negocios, 17(55), 1007-1020.
Riesgo, I. (2007). Sistemas de salud. Sistema sanitario español. En J. Villalobos Hidalgo (Ed.), Gestión sanitaria para profesionales de la salud (1.a ed., pp. 1-27). McGraw-Hill.
Roqué-Sánchez, M. V., & Gonzalvo-Cirac, M. (2015). Demografía, población vulnerable y Bioética. Persona y Bioética, 19(2), 245-263. https://doi.org/10.5294/pebi.2015.19.2.5.
Ruiz, J. (2018). Reflexión acerca del concepto de “Una salud”. Revista Peruana de Medicina Experimental y Salud Pública, 35(4), 657. https://doi.org/10.17843/rpmesp.2018.354.3821.
Sabando, P., & Rey del Castillo, J. (2020). ¿Uno o diecisiete sistemas de salud en España? En El Sistema Nacional de Salud: Pasado, presente y desafíos de futuro. Ediciones Díaz de Santos.
San Sebastián, A., & Barandiaran, K. (2022). Museo San Telmo: mapa de stakeholders desde la perspectiva de generación de valor social. En L. San-Jose & J. L. Retolaza (Eds.), Monetizando el valor social en la economía naranja. El caso de los museos vascos. ESIC.
Sandel, M. J. (2011). Justicia. ¿Hacemos lo que debemos? Debate.
San-Jose, L., & Retolaza, J. L. (2016). Contabilidad social orientada a los Stakeholders. Pirámide.
San-Jose, L., Retolaza, J. L., & Bernal, R. (2021). Índice de valor social añadido: una propuesta para analizar la eficiencia hospitalaria. Gaceta Sanitaria, 35(1), 21-27. https://doi.org/10.1016/j.gaceta.2019.08.011.
San-Jose, L., Retolaza, J. L., & Freeman, E. (2017). Stakeholder Engagement at Extanobe: A Case Study of the New Story of Business. Stakeholder Engagement: Clinical Research Cases, 285-310.
Stake, R. (2005). Investigación con estudios de caso. Madrid, Morata.
Sweeney, J. C., & Soutar, G. N. (2001). Consumer perceived value: The development of a multiple item scale. Journal of Retailing, 77(2), 203-220. https://doi.org/10.1016/S0022-4359(01)00041-0.
Tampio, K. P., Haapasalo, H., & Ali, F. (2022). Stakeholder analysis and landscape in a hospital project–elements and implications for value creation. International Journal of Managing Projects in Business, 15(8), 48-76.
Thadani, K., & Patnaik, M. (2023). Spain Healthcare Cooperatives: Inspiring Model for the Developing Countries. In World Healthcare Cooperatives: Challenges and Opportunities (pp. 137-152). Emerald Publishing Limited.
Yin, R. K. (2009). Case study research: Design and methods (4th Ed.). Thousand Oaks, CA: Sage.
Zarco, C. (2018). El cooperativismo sanitario es una tercera vía a la sanidad pública o privada. iSanidad.
Table Annex 1: Responsibility of the agents involved in the sustainability of the National Health System according to the Spanish Bioethics Committee.
|
Agent involved |
Keys to Responsibility |
|
Health professionals |
Inclusion of justice in the values that inspire health care. Responsibility for prescribing medication, diagnostic tests, sick leave, referrals or hospital stays. Criteria for allocating resources equitably and efficiently. Tendency towards defensive medicine which may increase healthcare costs. Curricula that include the sustainability of the NHS as an ethical and legal value. A climate of trust that improves the doctor-patient relationship and the adoption of conflict resolution formulas. Transparency and proper management of conflicts of interest and transparency. |
|
Politicians and managers |
Fragility of the structure of the NHS, strengthening the coordinating role of the Interterritorial Health Council. Unjustified inequality between Autonomous Communities (e.g. vaccination schedules, financing of medicines, lack of solidarity in treating patients from other neighbouring communities). Lack of transparent discussion on the services provided by each regional health service. Inequality and imbalance between resources for hospital care and primary care. Encourage dialogue and public deliberation to avoid unilateral decisions on resource allocation. Lack of continuity in projects to improve and modernise the NHS. Improving the evaluation and diagnosis of health policy. The professionalisation of the management function as an essential element for the responsible administration of economic, human and material resources at all levels of the NHS. Investment in the human capital of the NHS. In health care institutions, training and research need to be promoted with care. Favouring professional promotion and work-life balance. Greater transparency and accountability. Greater social participation. |
|
Citizens and patients |
Greater protagonism in decision-making in the NHS. Promote training in the proper use of health resources. Partnerships with citizens' associations. Optimise the use of NHS healthcare, especially where open access exists, More information on investment and disinvestment alternatives within the NHS and a greater role and participation in decision-making. Reflection on cost-opportunity, closely linked to distributive justice, in health education for NHS users as individual decisions have a direct impact on the collective. Responsible behaviour in the use of collective NHS resources (e.g. cancelling appointments). Although the promotion of healthy living and preventive activities supports the sustainability of the NHS, it should not be the individual who suffers from a disease that matters. It is not only lifestyle that plays a role, but also other factors such as genetic predisposition, socio-economic background or environmental setting. Support patient associations with public funding for their undoubted contribution to the NHS. |
|
NHS Providers |
Undoubted contribution to research through large investments in research, a very profitable sector in advanced countries. The high cost of new medicines and so-called "high technology" is one of the largest items of health spending, and is not always proportional to the health results obtained, putting the sustainability of the NHS under great strain. Justification the high prices of medicines as it requires long and costly processes, and there is controversy over the price margin that is dedicated to commercial promotion. Therefore, a rethinking of the sector, whose main client is the NHS, is called for. Industry conflicts of interest in the production and dissemination of knowledge and their influence on professionals, managers, scientific societies, patient associations or even governments. Call for cooperation and transparency in line with the Resolution on public health and the pharmaceutical industry of the Parliamentary Assembly of the Council of Europe (2015). Participation in a pact for the sustainability of the NHS, with co-responsibility and transparency that contributes to health policies aligned with the real needs of citizens. Avoiding the tendency to medicalisation. Submission of technological developments to the judgement of technology assessment committees, to be set up by the health authorities with guarantees of independence. |
|
Media and advertising |
They share a responsibility for the proper functioning of the NHS as a public service. New technologies and the media have a great influence on lifestyle and the socialisation of scientific information, with rigour in information being an essential issue in health care and even in the concept of health. Responsibility not to create sensationalism and false expectations about health. Seek scientific and medical advice in the creation of health content, being especially careful in the way it is conveyed. Health professionals should collaborate in this task of educating society about health. Health as a consumer good, as advertising is not always truthful, which has major consequences as the population can make decisions about their health. The need for scientific rigour, responsibility and legal standards to guarantee the protection of users. |
Source: own elaboration based on CBE
Table Annex 2: Value that patients recognized for that the case, then the hospital create for them.
|
Stakeholder |
Day |
Time |
Interview Type |
Value Variable-Contribution |
|
Pacient |
||||
|
Patients organization |
1/02/2023 |
30 m. |
Online |
Enhances public health Access to healthcare professionals Collaboration Emergency services Peace of mind |
|
Pacient 1 |
19/07/2023 |
20 m. |
In-person, provided room |
Emergency services Reduction of visits Quality of care Peace of mind Emission reduction |
|
Pacient 2 |
19/07/2023 |
30 m. |
In-person, provided room |
Quality of care Hospital infrastructure |
|
Pacient 3 |
07/10/2023 |
20 m |
In-person, provided room |
Emergency services Reduction of visits Quality of care Peace of mind Emission reduction |
|
Pacient 4 |
07/10/2023 |
20 m. |
In-person, provided room |
Emergency services Reduction of visits Quality of care Peace of mind Medical chat and video consultation |
|
Pacient 5 |
07/10/2023 |
20 m. |
In-person, provided room |
Shorter waiting lists No unnecessary waiting Reduction of visits Medical chat and video consultation |
Source: own elaboration.